![]()
![]()
Below are images of people that have had repair of major skin defects of various parts of th nose. Most are quite large and all required a local flap for closure. The postoperative images are taken with high magnification of the operative site so that all scarrs and possible blemishes are clearly visible. Under normal circumstances, the scars and evidence of surgery are even harder to find.
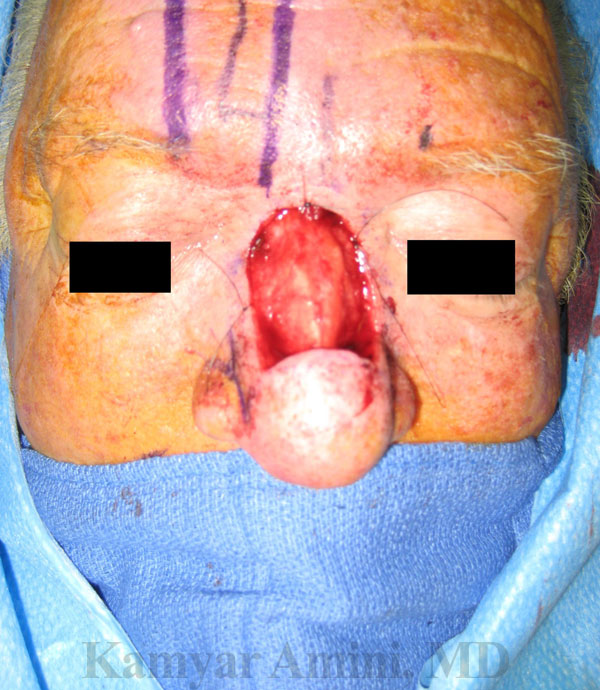
 This gentleman was referred by his Mohs surgeon for a very aggressive skin cancer called a Merkel Cell Carcinoma. He had all skin removed from the upper two thirds of his nose. The picture on the left shows the defect and the one on the right is the final appearance 6 months after a paramedian forehead flap (a flap of skin and muscle borrowed from the forehead) to close the wound. The profile view (coming soon) shows the excellent match of thickness of the flap with the native skin from the lower nose.
This gentleman was referred by his Mohs surgeon for a very aggressive skin cancer called a Merkel Cell Carcinoma. He had all skin removed from the upper two thirds of his nose. The picture on the left shows the defect and the one on the right is the final appearance 6 months after a paramedian forehead flap (a flap of skin and muscle borrowed from the forehead) to close the wound. The profile view (coming soon) shows the excellent match of thickness of the flap with the native skin from the lower nose.




These four pictures are before and after shots of a gentleman that lost his entire right nasal ala (nostril) to basal cell carcinoma skin cancer. He had a two staged melolabial transposition flap (skin and fat borrowed from the upper lip and cheek) on top of an auricular cartilage graft (cartilage borrowed from the ear for support). This involved rotating a paddle of skin into the defect which was left in place for three weeks. Once it had achieved a good blood supply, it was shaped into a new nostril. The cartilage borrowed from the ear was essential so that the new nostril would not collapse once the skin had healed. On the frontal view, you can see that the new nostril has a fairly normal curve and shape thanks to the deep cartilage that is now supporting it.

 This woman had an extremely aggressive and large squamous cell carcinoma skin cancer that resulted in loss of skin from the tip of the nose, the side of the nose, and the skin of the cheek. She was referred by her Mohs surgeon after he had removed the tumor for flap repair of this complex facial defect. She had repair with a paramedian forehead flap (skin and muscle rotated down from the forehead) in addition to a cheek advancement flap (skin pulled in from the normal surroinding cheek).
This woman had an extremely aggressive and large squamous cell carcinoma skin cancer that resulted in loss of skin from the tip of the nose, the side of the nose, and the skin of the cheek. She was referred by her Mohs surgeon after he had removed the tumor for flap repair of this complex facial defect. She had repair with a paramedian forehead flap (skin and muscle rotated down from the forehead) in addition to a cheek advancement flap (skin pulled in from the normal surroinding cheek).


This woman had nearly the entire left side and top of her nose removed for squamous cell carcinoma of the skin. She had a two stage paramedian forehead flap reconstruction. The purple markings in the picture on the left show where the forehead flap came from. This is a good example of why the forehead flap is such a good thickness and color match with the skin of the nose.


This woman had a superficial basal cell carcinoma skin cancer of the nasal tip. She had already undergone paramedian forehead flap repair of a separate lesion on the side of the nose so we chose to repair this smaller defect with a free skin graft. This came from behind the ear and gave a very good thickness match. You can still see how it is a little pale compared to the surrounding skin. This usually improves with time and has become much less visible since the taking of these pictures.


lorem


Gentleman with deep defect involving the upper part of the side of the nose and face after Mohs resection for basal cell carcinoma skin cancer. He was referred for complex repair by the Mohs surgeon. Due to the thickness of the defect, a flap reconstruction was necessary. This was followed by two minor scar revisions to achieve the appropriate thickness. The frontal view demonstrates this the best.

 Lorem ipsum
Lorem ipsum


This woman had a deep facial and nostril defect after removal of a basal cell carcinoma skin cancer. Although the defect is small compared to the others pictured above, it is deep and reached the inner aspect of the nasal cavity. This required internal repari in addition to external skin flap reconstruction.
|
Dr. K. Amini 8435 Reseda Blvd Northridge, CA 91324 |



@ ENT Doctor LA, Website was created and maintained by Biago Media